|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 3
| Issue : 2 | Page : 42-46 |
|
Repair of porcelain restorations: Four case reports
Hasan Hüseyin Kocaagaoglu Yrd. Doç.
Department of Prosthodontics, Faculty of Dentistry, Pamukkale University, Denizli, Turkey
| Date of Web Publication | 29-May-2015 |
Correspondence Address:
Dr. Hasan Hüseyin Kocaagaoglu
Department of Prosthodontics, Faculty of Dentistry, Pamukkale University, Denizli
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.157834

Porcelain has been used with prosthetic restorations for many years. Although their long term success has been demonstrated, failures may occur in metal-porcelain restorations due to trauma, laboratory failures or premature contacts. Damaged porcelain restorations can cause serious clinical and esthetic problems. In some situations, the production of a new restoration is difficult because of the high treatment costs. Porcelain repair may provide a practical alternative for patients and clinicians, especially those restorations with minor porcelain cracks. In the present series of case reports, repair of the fractured metal-porcelain restorations, using porcelain repair system and composite resin were demonstrated. Keywords: Composite resins, dental porcelain, dental restoration repair
How to cite this article:
Kocaagaoglu HH. Repair of porcelain restorations: Four case reports. Eur J Prosthodont 2015;3:42-6 |
| Introduction | |  |
Metal-porcelain restorations are regarded as the gold standard in fixed prosthodontic treatment. [1] Patients use well-designed restorations for several years without any problems. Studies have demonstrated lots of advantages of porcelain restorations, such as color stability, radiopacity, good compressive and abrasive resistance, and esthetics. [2]
However, problems which can result from patients (bruxism); from the laboratory (unsuitable infrastructure design and/or the use of a particular metal); and/or from dentists (incorrect tooth preparations) may be occur. Incorrect tooth preparations lead to poorly designed restorations resulting in issues such as broken connectors, and minor damage, such as chipping. [3] In the literature, veneering porcelain fractures have been defined as "chipping." [4] Delaminations with the exposure of core materials and minor chip-off fractures are mentioned as the most frequent reason for porcelain restoration failures. [5],[6],[7] Veneer chipping is reported more often with porcelain-fused-to-metal structures. [8] A fractured porcelain restoration poses esthetic and clinical problems. [9] The first option includes remake of the restoration and the other includes repair. However, remake of the restoration is not always possible because of the high treatment costs. Three situations are mentioned for repair of metal-porcelain restorations: (1) Fracture in porcelain only with no exposure of metal, (2) fracture with some exposure of metal, and (3) fracture with complete deveneering of porcelain exposure of metal. [10]
According to the literature, repair methods of the damaged restorations have been classified into 2 types, the indirect method, and the direct method. [9] Indirect repair is an option that includes repair of the restoration in the laboratory, [11],[12] while direct repairs include techniques that use composites applied directly to the fractured restoration. [12],[13]
If the damage is on a crown that is part of a precision attachment denture and/or implant supported denture, direct (intraoral) repair may be the most rational option. With the expanding use of porcelain systems, the need for porcelain restoration repair has been raised. [14]
The aim of this series of case reports is to establish that it is possible to regain a restoration's functional status using intraoral porcelain repair systems without removing the restoration in the case of minor damage.
| Case Reports | | |
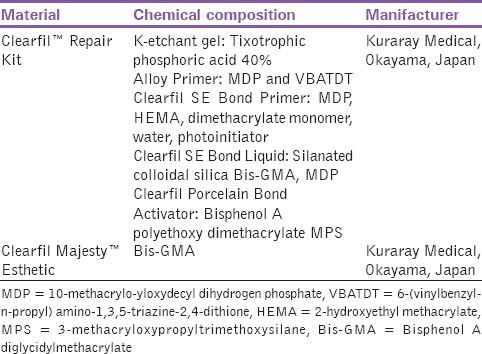
Four patients who had veneering porcelain fractures were referred to the Department of Prosthodontics, Erciyes University for their prosthetic evaluations. Intraoral examinations revealed minor porcelain fractures of the restorations. For all patients, intraoral repair of fractured restorations was planned. Clearfil™ Intraoral Porcelain Repair System (Kuraray Medical, Okayama, Japan) was used as the repair system for all patients [Table 1].
The application steps of the intraoral repair system include:
- Applied the acid etch with the application of 40% tixhotrophic phosphoric acid for 5 s, washed, and air dried;
- Applied the metal primer for 20 s and air dried;
- Mixed the porcelain bond activator and SE bond primer for 5 s;
- Applied the bonding agent for 10 s and photopolymerization for 40 s;
- Applied the opaquer photopolymerization for 40 s;
- Applied the composite resin (Clearfil Majesty Esthetic, Kuraray Medical, Okayama, Japan) photopolymerization for 40 s;
- Finished and polished.
Prior to the application steps, an intraoral sandblasting machine with 50-μm Al 2 O 3 of powder was used in order to roughen the surfaces of the restorations in all patients. In addition, all porcelain surfaces were beveled in order to achieve strong bond strengths and esthetics. [3] A rubber dam was used to protect the intraoral tissues from the effects of etching and sandblasting.
Case 1
A 53-year-old female patient applied to the clinic for the rehabilitation of her fractured restoration. Upon intraoral examination, a mandibular removable partial denture was noted which utilized two metal-porcelain crowns with rest seats. The mandibular left premolars had crowns with a fracture of the mesio-occlusal surface. The restoration had been completed about 1-year previously. The patient refused the removal of her fixed restoration. Therefore, the restoration was repaired intraorally. The patient was satisfied with the treatment [Figure 1] and [Figure 2]. | Figure 1: Occlusal view of the block crown with a crack of the mesio-occlusal part
Click here to view |
Case 2
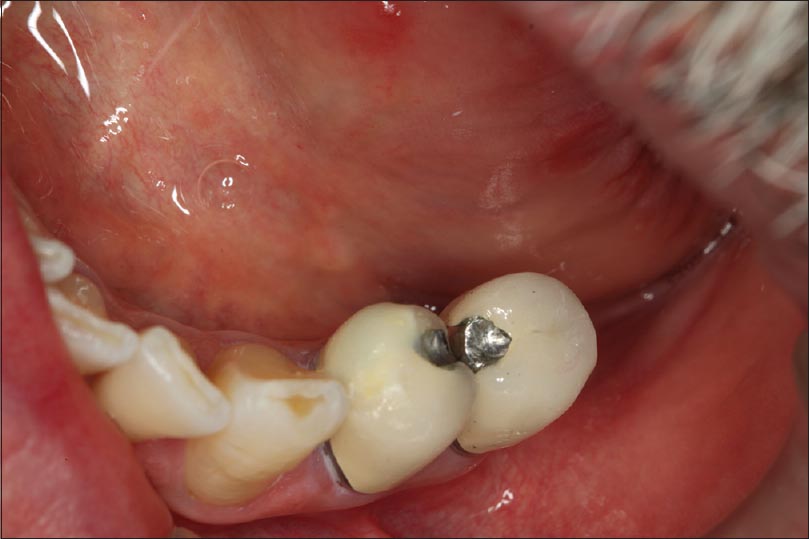
A 48-year-old male patient has a 4-unit metal-porcelain fixed partial denture with good marginal adaptation. The patient's chief complaint was that the porcelain had chipped from the metallic structure in the mandibular second molar tooth most likely due to a premature contact. The patient refused replacement of the fixed partial denture. In addition, the restoration had a good marginal adaptation. Thus, as a treatment option, porcelain repair was selected, and the restoration was repaired intraorally [Figure 3] and [Figure 4]. | Figure 3: Clinical view of the chipped porcelain in the distal surface of the mandibular right second molar
Click here to view |
Case 3
A 56-year-old female patient with a 7-unit metal-porcelain fixed partial denture, which was 18 months old, presented with fractured porcelain from the metallic structure in the maxillary left canine. In addition, the patient had a removable partial denture whose retentive crown had been damaged during the restoration. For financial reasons, the patient refused the denture replacement. Therefore, the restoration was repaired intraorally [Figure 5] and [Figure 6]. | Figure 5: View of the case with a fractured porcelain in the mesio-buccal surface of the maxillary left canine
Click here to view |
Case 4
A 49-year-old female patient with a 1-year old 3-unit metal-porcelain fixed partial denture presented with porcelain fractured from the metallic structure in the mandibular first premolar tooth. The restoration had a good marginal fit, and the gingival tissue was periodontally healthy. Treatment options were explained to the patient and the patient selected repair of the restoration intraorally. The patient was satisfied with the treatment [Figure 7] and [Figure 8]. | Figure 7: View of the fractured porcelain in the buccal surface of the mandibular left first premolar
Click here to view |
| Discussion | | |
These series of case reports demonstrate the repair of metal-porcelain restorations with composite resin. While porcelain restorations have been used for several years in dental treatments, restoration fracture or breakage may occur as a result of issues created by the laboratory, patient, or dentist. [10] When a crack occurs in a restoration, there are two possible solutions: The first is to remake the restoration and the second is to repair the restoration. Especially in minor cases, such as chipping of the porcelain, a repair should be considered because it is more economical. [15]
In the literature, although there are several in vitro studies about the repair of porcelain restrations, [1],[7],[10],[12],[13],[14] only few case studies are available. [3],[9]
There are many systems developed for this purpose. Advances in adhesive systems and restorative materials have enabled the development of intraoral repair systems. Before the repair of any restoration, the reason for the fracture should be investigated and eliminated in order to ensure successful treatment. [14],[16]
It is important to provide durable chemical and micromechanical bonds between dental porcelain and composite resin. [3] In this case, mechanical retention was promoted through the use of beveled surfaces on the porcelain created using diamond burs and sandblasting. It has been reported that roughening the surface of exposed metal or porcelain using sandblasting provides good results. [17]
Actually, the long term successful results depend on the correct and careful application of the bonding techniques and excellent occlusal adjustment. [3] The resin bonding is adversely affected by contamination of fluids. [18] For this reason, any contaminants should be eliminated before bonding procedures. [19]
Acid etching was applied to clean and roughen the surface to be treated because the bonding surface may be contaminated with saliva, which results in reduced bond strength.
In addition, for control of the oral cavity fluid, a rubber dam was used in all treatments. Therefore, the bonding area was protected. Achieving moisture control is difficult, when rubber dam isolation is impossible. [18]
For exposed metal surfaces, a metal primary agent (Alloy Primer, Kuraray Medical, Okayama, Japan) was applied in order to increase the bond strength of the composite resin to the surface. In the literature, there are numerous studies about metal primary agents. [20],[21]
After the etching, abrasion, and the application of the metal primary agent process, a silane coupling agent was applied to the surface in order to achieve high bond strengths. Silane coupling agents are conducive to covalent bond formation between the porcelain surface and the composite, and they also improve the wetting of the porcelain surface for the bonding. [22]
In all cases, after the repair process, composite surface was polished using a two-step polishing system (Engance ® and PoGo ® , Dentsply Caulk, Milford, DE, USA). The quality of the polishing technique affects the longevity and esthetic appearance of dental materials. [23] High-quality polishing improve both the esthetics and the longevity of composite restorations. In addition, poorly polished surfaces contribute to plaque accumulation, gingival irritation and discoloration of the restoration that may lead to patient dissatisfaction and additional expense for a replacement. [24],[25]
Repaired restorations should be resistant to breakage, and to this end, several precautions should be taken, such as eliminating premature contacts.
In the present study, intraoral porcelain repairs were demonstrated. The patients' restorations were treated with a porcelain repair system and composite resin. Dental professionals can use acceptable repair techniques that are simple, economical and quick for such restorations. [17] One deficiency in this study was the lack of the use of tribochemical silica coating, but this can be resolved in future case studies.
| Summary | | |
These clinical report series described the intraoral repair of metal-porcelain restorations using composite resin. The repair of porcelain restorations can be an esthetic and functional alternative for patients and dentists. Therefore, dental clinicians should be able to repair porcelain restorations intraorally under appropriate conditions.
| References | | |
| 1. | dos Santos JG, Fonseca RG, Adabo GL, dos Santos Cruz CA. Shear bond strength of metal-ceramic repair systems. J Prosthet Dent 2006;96:165-73.  |
| 2. | Pameijer CH, Louw NP, Fischer D. Repairing fractured porcelain: How surface preparation affects shear force resistance. J Am Dent Assoc 1996;127:203-9. |
| 3. | Raposo LH, Neiva NA, da Silva GR, Carlo HL, da Mota AS, do Prado CJ, et al. Ceramic restoration repair: Report of two cases. J Appl Oral Sci 2009;17:140-4. |
| 4. | Mainjot AK, Schajer GS, Vanheusden AJ, Sadoun MJ. Residual stress measurement in veneering ceramic by hole-drilling. Dent Mater 2011;27:439-44. |
| 5. | Raigrodski AJ, Chiche GJ, Swift EJ Jr. All-ceramic fixed partial dentures, Part III: Clinical studies. J Esthet Restor Dent 2002;14:313-9. |
| 6. | Sailer I, Pjetursson BE, Zwahlen M, Hämmerle CH. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part II: Fixed dental prostheses. Clin Oral Implants Res 2007;18 Suppl 3:86-96. |
| 7. | Lee SJ, Cheong CW, Wright RF, Chang BM. Bond strength of the porcelain repair system to all-ceramic copings and porcelain. J Prosthodont 2014;23:112-6. |
| 8. | Pjetursson BE, Brägger U, Lang NP, Zwahlen M. Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin Oral Implants Res 2007;18 Suppl 3:97-113. |
| 9. | Galiatsatos AA. An indirect repair technique for fractured metal-ceramic restorations: A clinical report. J Prosthet Dent 2005;93:321-3. |
| 10. | Gourav R, Ariga P, Jain AR, Philip JM. Effect of four different surface treatments on shear bond strength of three porcelain repair systems: An in vitro study. J Conserv Dent 2013;16:208-12. [ PUBMED]  |
| 11. | Helpin ML, Fleming JE. Laboratory technique for the laminate veneer restoration. Pediatr Dent 1982;4:48-50. |
| 12. | Fahmy NZ, Mohsen CA. Assessment of an indirect metal ceramic repair system. J Prosthodont 2010;19:25-32. |
| 13. | Kupiec KA, Wuertz KM, Barkmeier WW, Wilwerding TM. Evaluation of porcelain surface treatments and agents for composite-to-porcelain repair. J Prosthet Dent 1996;76:119-24. |
| 14. | Blum IR, Nikolinakos N, Lynch CD, Wilson NH, Millar BJ, Jagger DC. An in vitro comparison of four intra-oral ceramic repair systems. J Dent 2012;40:906-12. |
| 15. | Chadwick RG, Mason AG, Sharp W. Attempted evaluation of three porcelain repair systems - What are we really testing? J Oral Rehabil 1998;25:610-5. |
| 16. | Kumbuloglu O, User A, Toksavul S, Vallittu PK. Intra-oral adhesive systems for ceramic repairs: A comparison. Acta Odontol Scand 2003;61:268-72. |
| 17. | Bagis B, Ustaomer S, Lassila LV, Vallittu PK. Provisional repair of a zirconia fixed partial denture with fibre-reinforced restorative composite: A clinical report. J Can Dent Assoc 2009;75:133-7. |
| 18. | Eiriksson SO, Pereira PN, Swift EJ Jr, Heymann HO, Sigurdsson A. Effects of saliva contamination on resin-resin bond strength. Dent Mater 2004;20:37-44. |
| 19. | Zhang S, Kocjan A, Lehmann F, Kosmac T, Kern M. Influence of contamination on resin bond strength to nano-structured alumina-coated zirconia ceramic. Eur J Oral Sci 2010;118:396-403. |
| 20. | Ikemura K, Tanaka H, Fujii T, Deguchi M, Endo T, Kadoma Y. Development of a new single-bottle multi-purpose primer for bonding to dental porcelain, alumina, zirconia, and dental gold alloy. Dent Mater J 2011;30:478-84. |
| 21. | Azimian F, Klosa K, Kern M. Evaluation of a new universal primer for ceramics and alloys. J Adhes Dent 2012;14:275-82. |
| 22. | Berry T, Barghi N, Chung K. Effect of water storage on the silanization in porcelain repair strength. J Oral Rehabil 1999;26:459-63. |
| 23. | Türkün LS, Türkün M. The effect of one-step polishing system on the surface roughness of three esthetic resin composite materials. Oper Dent 2004;29:203-11. |
| 24. | Yalçin F, Korkmaz Y, Baseren M. The effect of two different polishing techniques on microleakage of new composites in Class V restorations. J Contemp Dent Pract 2006;7:18-25. |
| 25. | Güler AU, Duran I, Yücel AÇ, Ozkan P. Effects of air-polishing powders on color stability of composite resins. J Appl Oral Sci 2011;19:505-10. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8]
[Table 1]
|












 Search Pubmed for
Search Pubmed for