|
| Article Access Statistics | | | Viewed | 678 | | | Printed | 17 | | | Emailed | 0 | | | PDF Downloaded | 3 | | | Comments | [Add] | | | Cited by others | 1 | | |
|


Click on image for details.
|
|
| |


 |
| Year : 2013 | Volume
: 7
| Issue : 4 | Page : 153-154 |
|
|
|
|
|
LETTER TO THE EDITOR Clavicle diaphyseal fracture, ipsilateral type 3 acromioclavicular joint dislocation stabilized with double plate
Ozan Beytemür, Oktay Adanir, Yasar Mahsut Dinçel, Mehmet Ali Baran, Mehmet Akif Güleç
Department of Orthopedics and Traumatology, Bagcilar Training and Research Hospital, Mimar Sinan Cad, Bagcilar, Istanbul, Turkey
Correspondence Address:
Ozan Beytemür
Department of Orthopedics and Traumatology, Bagcilar Training and Research Hospital, Mimar Sinan Cad, 6, sok.34200, Bagcilar, Istanbul
Turkey
 Source of Support: None, Conflict of Interest: None  | 1 |
DOI: 10.4103/0973-6042.123536

|
|
|
|
| Date of Web Publication | 24-Dec-2013 |
How to cite this article:
Beytemür O, Adanir O, Dinçel YM, Baran MA, Güleç MA. Clavicle diaphyseal fracture, ipsilateral type 3 acromioclavicular joint dislocation stabilized with double plate. Int J Shoulder Surg 2013;7:153-4 |
Sir,
Clavicle diaphyseal fractures and acromioclavicular (AC) joint dislocation injuries are often seen separately. Clavicle medial third shaft fracture combined with ipsilateral acromioclavicular joint dislocation is a rarely seen injury type. [1],[2],[3],[4] There are 9 cases published in literature. There is only a case of Rockwood type 3 AC joint injury combined with clavicle shaft fracture.
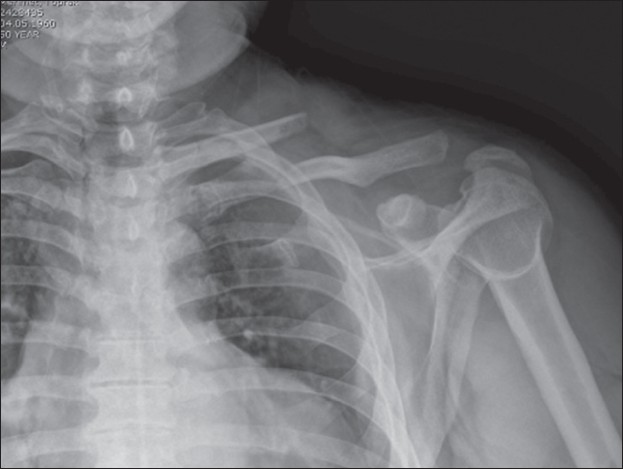
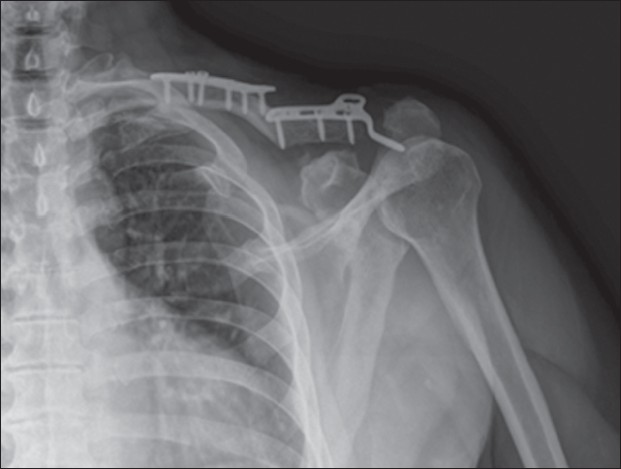
A 50-year-old male patient was admitted to Emergency department, after a motor vehicle accident. The mechanism of trauma is a blunt force on left shoulder, as the vehicle lied on the left side. The examination findings were swelling, tenderness, ecchymosis and limitation of the left shoulder movements. No neurovascular injury was diagnosed. The result of clinical and radiological examination was fracture of the first and second costa, fracture of the middle third of the left clavicle and ipsilateral type 3 AC joint dislocation according to Rockwood classification [Figure 1] and [Figure 2]. The patient was operated one day after the trauma. Operations were performed under general anesthesia, in beach chair position, with a transverse incision. After reaching the fracture line and performing the reduction, osteosynthesis was obtained using a low profile anatomic plate with six holes and screws. Then the incision was elongated to reach the AC joint. AC disc was dislocated and injured. After the disc excision, the joint was fixed with a 4 hole clavicular hook plate and 3 screws. A sling was worn for two weeks postoperatively. Rehabilitation was started by passive assisted movements at postoperative first week; all active shoulder movements were permitted at postoperative fourth week. Strengthening exercises were performed between 8 and 12 weeks and at the end of 12th week all the movements were full and painless. At the 23rd month examination all shoulder movements were full and painless and widening of the AC joint space and degenerative findings were seen in direct radiographs [Figure 3]. We did not remove the clavicle hook plate because the patient did not complain.
The treatment of this rarely seen injury is controversial. Heinz et al. reported a case of bike rider treated conservatively. At 24-month follow-up, the patient was clinically well, despite of radiologically dislocated AC joint. [1] | Figure 2: Three-dimensional computed tomography image of the left shoulder
Click here to view |
Wurtz et al. reported 4 cases of this combined type. They treated surgically 3 cases of type 4AC dislocation and, conservatively 1 case with type 2 AC joint dislocation. All cases were treated successfully. [2] John et al. reported a 21-year-old hockey player with combined medial fracture and type VI AC joint dislocation case. This conservatively treated patient returned to hockey 14 weeks after trauma. [3]
Pasarkis et al. reported surgically treated clavicle medial third fracture and Rockwood type 5 AC joint injury. They used stabilization with anatomic plate and tightrope fixation system for AC joint injury and 18 months follow-up results were successful. [4]
In literature there are successful results with both conservative and surgical treatments. In conclusion, although fixation with double plate results in a painless shoulder, due to radiological abnormalities seen at the follow-up graphics, coracoclavicular screw, endobutton plate together with clavicle anatomic plate may be an alternative treatment choice. Also we need more cases and longer follow-up periods for giving an absolute decision about the treatment method of these combined type injuries.
 References References | |  |
| 1. | Heinz WM, Misamore GW. Mid-shaftfracture of the clavicle with grade III acromioclaviculer seperation. J Shoulder Elbow Surg1995;4:141-2. 
[PUBMED] |
| 2. | Wurtz LD ,Lyons FA, Rockood CA Jr. Fracture of the middle third of the clavicle and dislocation of the acromioclaviculer joint. J Bone JointSurg Am1992;74:133-7.
|
| 3. | John MS, Simonian PT. Tip VI acromioclaviculer seperation with middle -third clavicle fracture in an ice hokey player.Clin J Sport Med2002;12:315-7.
|
| 4. | Psarakis SA, Savvidou OD, Voyaki SM, Beltsios M, Kouvaras JN. A rare injury of ipsilateral mid-third clavicle fracture with acromioclavicular joint dislocation. Hand (N Y) 2011;6:228-32.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3]
| This article has been cited by | | 1 |
Surgical Management of Acromioclavicular Dislocations |
|
| Jay B. Cook,John M. Tokish | | Clinics in Sports Medicine. 2014; 33(4): 721 | | [Pubmed] | [DOI] | |
|
|
|
|
|